Biotin
CAS number: 58-85-5
Biotin is necessary for formation of fatty acids and glucose, which are used as fuels by the body.
Related images
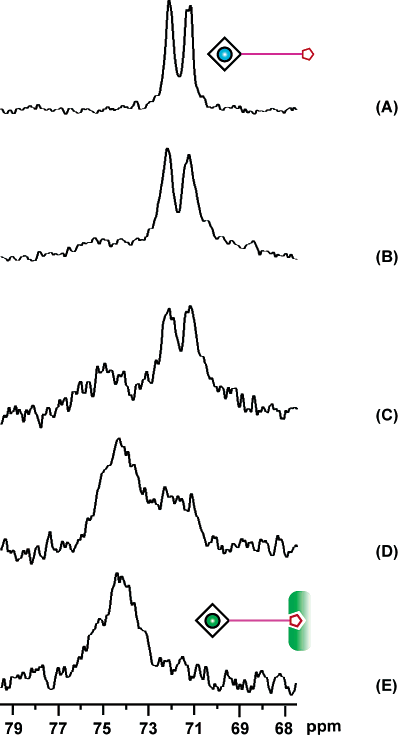
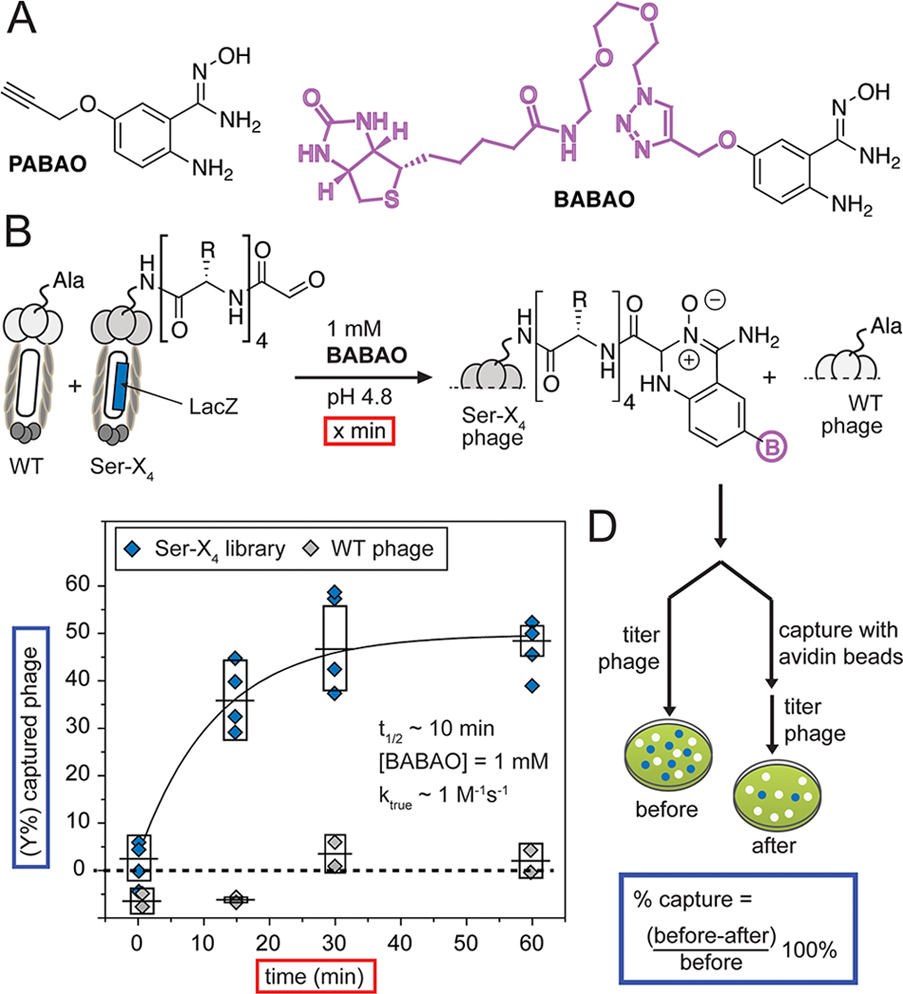
(A) Structures of ABAO derivatives that contain propargyloxy group and biotin. (B) Quantification of the reaction of BABAO with the M13 phage displaying a library of peptides with N-terminal glyoxal and wt phage displaying no aldehyde (1011 PFU/mL each). (C) Phage mixture was exposed to BABAO for the specified time. (D) To measure the reaction rate, we exposed the mixture of phage to 1 mM BABAO and measured biotinylation as a function of time by avidin capture. Error bars represent standard deviations from four independent kinetics experiments.
Related Questions and Answers
A: High circulating biotin from supplements can block streptavidin/avidin binding sites, yielding false-negative or false-positive results in assays such as IMMULITE-2000 or NOVEOS; ImmunoCAP systems are unaffected because they do not use biotin–streptavidin bridges. Patients should therefore stop biotin supplementation 48 h (or longer at high doses) before blood collection for such tests.
A: Experimental data show that biotin deficiency in mice increases susceptibility to nickel contact hypersensitivity via elevated IL-1β production, whereas high serum biotin levels correlate weakly with increased total and specific IgE in children, suggesting both deficiency and excess can dysregulate immune responses and potentially promote allergy.
A: Documented hypersensitivity to biotin itself is extremely rare; only two published occupational cases describe contact allergy to biotin or its synthetic precursors, and no cases have been reported from dietary, cosmetic, or therapeutic use of biotin.
A: The imidazolidine fragment of the biotin molecule binds with high affinity to avidin (a glycoprotein in egg white) and streptavidin (a tetrameric protein from Streptomyces avidinii), forming the basis for biotin–(strept)avidin bridging systems used in immunoassays.
A: Biotin is stable at pH 4–9, withstands high temperatures (melting point 229–232 °C), does not decompose under sunlight, and at room temperature is an odorless white crystalline powder or colorless crystals.
A: Biotin is a heterocyclic organic chemical compound with a system of condensed imidazolidine and thiolate rings attached to an alkyl chain terminated by a carboxyl group (valeric acid chain). Its molecular formula is C₁₀H₁₆N₂O₃S and only the D-(+)-biotin isomer is biologically active.